The Burden of Health Disparities Continues to Affect Disproportionately Which Population S
Introduction
The disparate impacts of the COVID-19 pandemic, ongoing incidents of police brutality, and recent rise in Asian hate crimes have brought health and health care disparities into sharper focus among the media and public. However, health and health care disparities are not new. They have been documented for decades and reflect longstanding structural and systemic inequities rooted in racism and discrimination. Addressing these inequities could help to mitigate the disparate impacts of the COVID-19 pandemic and prevent further widening of health disparities going forward. Moreover, narrowing health disparities is key to improving our nation's overall health and reducing unnecessary health care costs. This brief provides an introduction to what health and health care disparities are, the status of disparities and how COVID-19 has affected them, the broader implications of disparities, and current federal efforts to advance health equity.
What are health and health care disparities?
Health and health care disparities refer to differences in health and health care between groups that stem from broader inequities. There are multiple definitions of health disparities. Healthy People 2020 defines a health disparity as, "a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage" and notes that disparities, "adversely affect groups of people who have systematically experienced greater obstacles to health based on their racial or ethnic group; religion; socioeconomic status; gender; age; mental health; cognitive, sensory, or physical disability; sexual orientation or gender identity; geographic location; or other characteristics historically linked to discrimination or exclusion." The Centers for Disease Control and Prevention (CDC) identifies health disparities as, "preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations." A health care disparity typically refers to differences between groups in health insurance coverage, access to and use of care, and quality of care. The terms "health inequality" and "inequity" also are used to refer to disparities. Racism, which CDC defines as the structures, policies, practices, and norms that assign value and determine opportunities based on the way people look or the color of their skin, results in conditions that unfairly advantage some and disadvantage others, placing people of color at greater risk for poor health outcomes.
Health equity generally refers to individuals achieving their highest level of health through the elimination of disparities in health and health care. Healthy people 2020 defines health equity as the attainment of the highest level of health for all people, and notes that it requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and health and health care disparities. CDC defines the achievement of health equity as when every person has the opportunity to "attain his or her full health potential" and no one is "disadvantaged from achieving this potential because of social position or other socially determined circumstances."
A broad array of factors within and beyond the health care system drive disparities in health and health care (Figure 1). Though health care is essential to health, research shows that health outcomes are driven by multiple factors, including underlying genetics, health behaviors, social and environmental factors, and access to health care. While there is currently no consensus in the research on the magnitude of the relative contributions of each of these factors to health, studies suggest that health behaviors and social and economic factors, often referred to as social determinants of health, are the primary drivers of health outcomes and that social and economic factors shape individuals' health behaviors. Moreover, racism negatively affects mental and physical health both directly and by creating inequities across the social determinants of health.
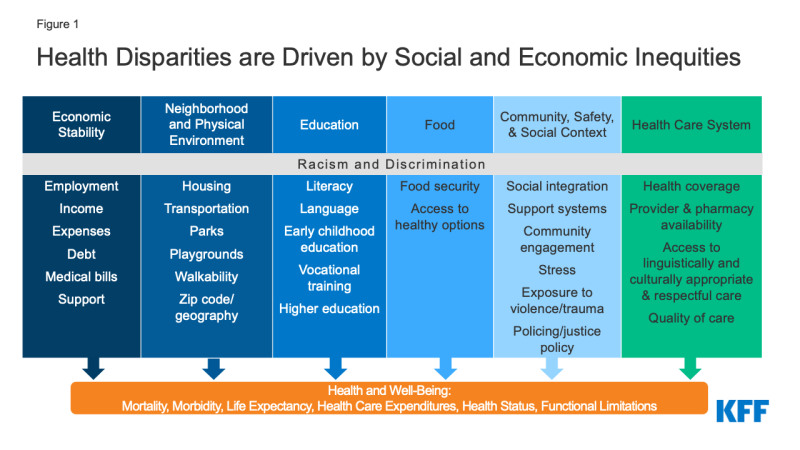
Figure 1: Health Disparities are Driven by Social and Economic Inequities
Health and health care disparities are often viewed through the lens of race and ethnicity, but they occur across a broad range of dimensions. For example, disparities occur across socioeconomic status, age, geography, language, gender, disability status, citizenship status, and sexual identity and orientation. Research also suggests that disparities occur across the life course, from birth, through mid-life, and among older adults.1 , 2 Federal efforts to reduce disparities focus on designated priority populations, including people of color, low-income populations, women, children/adolescents, older adults, individuals with special health care needs, and individuals living in rural and inner-city areas. These groups are not mutually exclusive and often intersect in meaningful ways. Disparities also occur within subgroups of populations. For example, there are differences among Hispanics in health and health care based on length of time in the country, primary language, and immigration status.3 , 4 Moreover, data for Asian people often mask underlying disparities among subgroups within the Asian population.5
What is the status of disparities?
Prior to the COVID-19 pandemic, people of color and other underserved groups faced longstanding disparities in health. Major recognition of health disparities began nearly two decades ago with two Surgeon General's reports published in the early 2000s that documented disparities in tobacco use and access to mental health care by race and ethnicity. Despite the recognition and documentation of disparities for decades and overall improvements in population health over time, many disparities have persisted, and, in some cases, widened.6 Recent data from before the COVID-19 pandemic showed that people of color fared worse compared to their White counterparts across a range of health measures, including infant mortality, pregnancy-related deaths, prevalence of chronic conditions, and overall physical and mental health status (Figure 2). As of 2018, life expectancy among Black people was four years lower than White people, with the lowest expectancy among Black men. Research also documents disparities across other factors. For example, low-income people report worse health status than higher income individuals,7 and lesbian, gay, bisexual, and transgender (LGBT) individuals experience certain health challenges at increased rates.
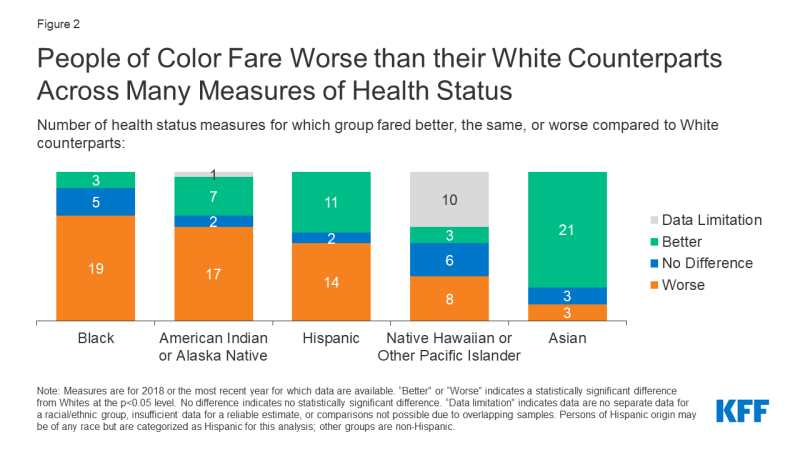
Figure 2: People of Color Fare Worse than their White Counterparts Across Many Measures of Health Status.
There also are longstanding disparities in health care. The Affordable Care Act health coverage expansions led to large gains in coverage across groups. Despite these gains, however, people of color and low-income individuals remain at increased risk of being uninsured (Figure 3), contributing to greater barriers to accessing health care. Further, starting in 2017, coverage gains stalled and began reversing, reflecting a range of actions by the Trump administration, including decreased funding for outreach and enrollment assistance, approval of state waivers to add new eligibility restrictions for Medicaid coverage, and immigration policy changes that increased fears among immigrant families about participating in Medicaid and CHIP. These coverage losses eroded some of the previous coverage gains under the ACA, particularly among Hispanic people, who already were at increased risk of being uninsured. Coverage losses have likely continued due to the COVID-19 pandemic as people have lost jobs and experienced declining income. Beyond disparities in coverage, people of color and lower income individuals also receive poorer quality of care. Recent KFF/The Undefeated survey data find that Black adults are more likely than White adults to report certain negative health care experiences, such as a provider not believing them and refusing them a test, treatment, or pain medication they thought they needed.
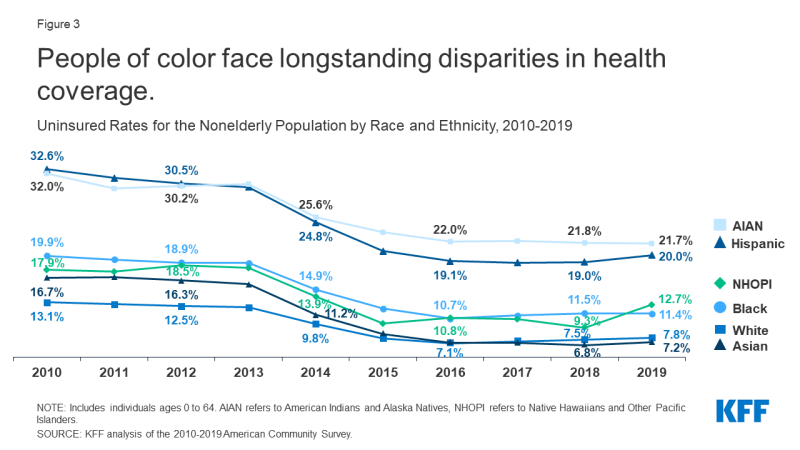
Figure 3: People of color face longstanding disparities in health coverage.
How has the COVID-19 pandemic affected disparities?
Data consistently show that American Indian and Alaska Native (AIAN), Black, and Hispanic people have experienced disproportionate rates of illness and death due to COVID-19 (Figure 4). Analysis further finds that AIAN, Black, Native Hawaiian and Other Pacific Islander (NHOPI), and Hispanic people had over three times premature excess deaths per 100,000 people in the US in 2020 than the rate among White or Asian people. The higher rates of illness and death among people of color reflect increased risk of exposure to the virus due to living, working, and transportation situations, increased risk of experiencing serious illness if infected due to higher rates of underlying health conditions, and increased barriers to testing and treatment due to existing disparities in access to health care.
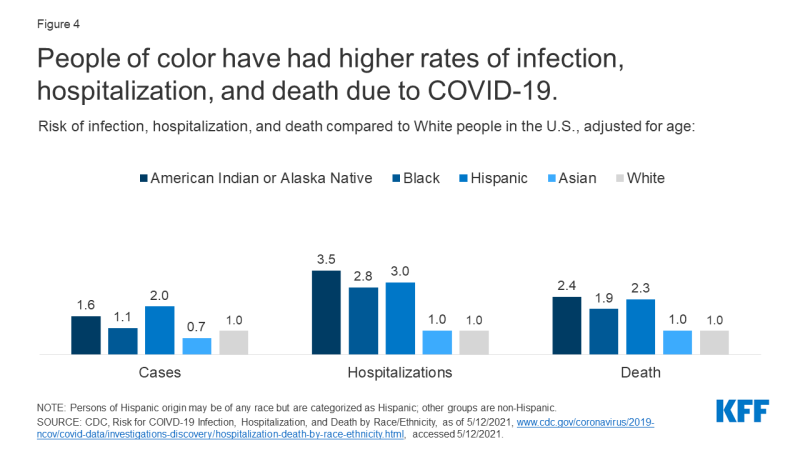
Figure 4: People of color have had higher rates of infection, hospitalization, and death due to COVID-19.
Beyond the direct health impacts of the virus, the pandemic has taken a disproportionate toll on the financial security and mental health and well-being of people of color, low-income people, LGBT people , and other underserved groups. For example, KFF survey data from February 2021, showed that about six in ten Hispanic adults (59%) and about half of Black adults (51%) said their household lost a job or income due to the pandemic, compared to about four in ten White adults (39%) who say the same. Moreover, adults with a household income under $40,000 were three times as likely as those with a household income of $90,000 or more to say they have had trouble paying for basic living expenses in the last three months (55% vs. 19%). As of late March 2021, Black and Hispanic adults were more likely than White adults to report lack of confidence in their ability to make their next housing payment and to report food insufficiency.
Despite being disproportionately affected by the pandemic, as of April 2021, Black and Hispanic people were less likely than White people to have received a COVID-19 vaccine. Data across states show a consistent pattern of Black and Hispanic people receiving smaller shares of vaccinations compared to their shares of cases, deaths, and the total population, resulting in lower vaccination rates compared to their White counterparts. While vaccination rates are increasing across all groups, the gaps in vaccination rates for Black and Hispanic people are persisting (Figure 5). These disparities in vaccinations reflect the longstanding inequities that create increased barriers to health care for people of color and other underserved groups. Moreover, they leave people of color at increased risk for infection and illness and hinder efforts to achieve population level immunity.
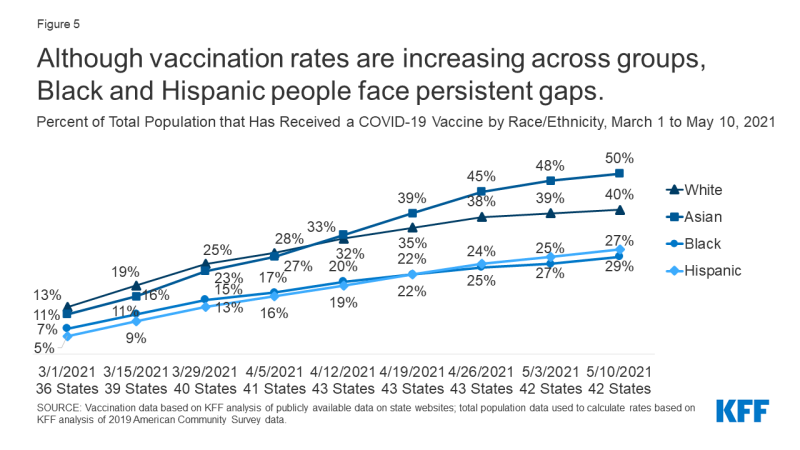
Figure 5: Although vaccination rates are increasing across groups, Black and Hispanic people face persistent gaps.
What are the broader implications of disparities?
Addressing disparities in health and health care is important not only from and social justice and equity standpoint, but also for improving the nation's overall health and economic prosperity. People of color and other underserved groups experience higher rates of illness and death across a wide range of health conditions, limiting the overall health of the nation. Research further finds that health disparities are costly. Analysis estimates that disparities amount to approximately $93 billion in excess medical care costs and $42 billion in lost productivity per year as well as additional economic losses due to premature deaths. As the population becomes more diverse, with people of color projected to account for over half of the population by 2050 (Figure 5), it is increasingly important to address disparities.
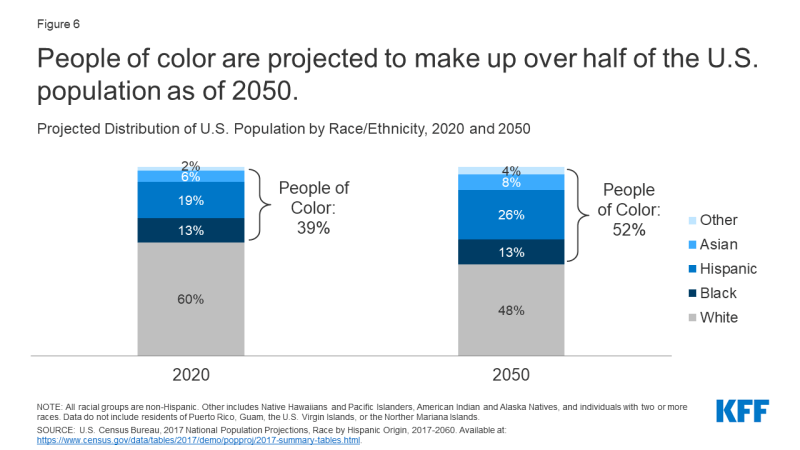
Figure 6: People of color are projected to make up over half of the U.S. population as of 2050.
The COVID-19 pandemic has exacerbated underlying disparities in health and health care and increased the importance of addressing them. This disparate impacts of the COVID-19 pandemic for people of color and other underserved groups may lead to even further widening of health disparities and greater health risks for the community as a whole, particularly if some groups remain at increased risk from COVID-19 due to lower vaccination rates and/or increased risk of exposure to the virus. As such, prioritizing equity in COVID-19 response efforts is not only important for mitigating the disproportionate impacts of the pandemic itself, but for protecting against even larger health disparities in the future.
What are current federal efforts to address health disparities?
The Biden administration has identified racial equity, including health equity, as a key priority , which has been reflected in several recent agency actions. Immediately after taking office, President Biden issued a series of executive orders and actions focused on advancing health equity. These included orders that outline equity as a priority for the federal government broadly and as part of the pandemic response and recovery. Reflecting the prioritization of health equity, in March 2021, the National Institutes of Health (NIH), launched the UNITE Initiative to address structural racism and racial inequities in biomedical research. In early April 2021, the Centers for Disease Control and Prevention (CDC) declared racism a serious threat to the public's health and noted that it would lead in efforts to confront systems and policies that have resulted in the generational injustice that has given rise to racial and ethnic health inequities. The Department of Health and Human Service's (HHS's) Office of Minority Health is focused on the "success, sustainability, and spread of health equity promoting policies, programs, and practices," and has three overarching programmatic priorities for FY2020 and 2021, including supporting states, territories, and tribes in identifying and sustaining health equity-promoting policies, programs, and practices; expanding the utilization of community health workers to address health and social service needs within communities of color, and strengthening cultural competence among healthcare providers throughout the country.
Federal COVID-19 response efforts have included a focus on equity. In January 2021, President Biden issued an Executive Order on Ensuring an Equitable Pandemic Response and Recovery to address the disproportionate and severe impact of COVID-19 on communities of color and underserved populations. The order establishes a COVID-19 Health Equity Task Force, directs agencies to strengthen equity data collection and reporting and ensure response plans and policies provide for equitable allocation of resources, and directs HHS to conduct an outreach campaign focused on building vaccine confidence among communities of color and other underserved populations. The COVID-19 relief American Rescue Plan Act, enacted in March 2021, provides new funding to support COVID-19 vaccination and other public health efforts, with a focus on enhancing access to vaccines and resources to protect against and respond to COVID-19 among underserved populations. In part, through this funding, HHS will invest nearly $10 billion to expand access to vaccines and better serve communities of color, rural areas, low-income populations, and other underserved communities. This includes $6 billion that will be provided to community health centers, which data show have been vaccinating larger shares of people of color compared to overall vaccination efforts.
The administration and Congress have taken a range of actions to expand access to and enrollment in health coverage. As noted, beginning in 2017, health coverage gains stalled and began reversing. The COVID-19 pandemic has likely further increased coverage losses as people have experienced job loss and decreases in income. In January 2021, President Biden issued an Executive Order on Strengthening Medicaid and the Affordable Care Act, which established a Special Open Enrollment Period for the Health Insurance Marketplaces and directed federal agencies to review policies and practices to ensure they support access to health coverage. The American Rescue Plan Act also contains provisions designed to increase access to health coverage and make health coverage more affordable. These include increases and expansions in eligibility for subsidies to buy health insurance through the Marketplaces as well as Medicaid provisions that offer incentives to encourage states that have not yet adopted the ACA Medicaid expansion to do so and provide a new option for states to extend the length of Medicaid coverage for postpartum women. The administration also restored funding for navigators to help eligible people enroll in health coverage and increased outreach activities. These actions will particularly benefit people of color and low-income people who are more likely to be uninsured. Six in ten uninsured adults who would become eligible if all remaining states expanded Medicaid are people of color, and over seven in ten are adults living below poverty. Overall, research shows that Medicaid expansion is associated with reductions in racial/ethnic disparities in health coverage as well as narrowed disparities in health outcomes for Black and Hispanic individuals, particularly for measures of maternal and infant health.
The administration has reversed policies implemented under the Trump administration that contributed to reduced access to health care and other programs for immigrant families. In February 2021, President Biden issued an Executive Order on Restoring Faith in Our Legal Immigration Systems and Strengthening Integration and Inclusion Efforts for New Americans, which declared that the federal government should develop welcoming strategies that promote integration, inclusion, and citizenship. The order directed federal agencies to review existing actions to ensure they are consistent with this policy, reduce barriers that impede access to immigration benefits, and review changes to public charge policies made under the Trump Administration, which contributed to reduced access to health care and other programs for immigrant families. The administration subsequently took action to reverse these public charge policy changes. The Department of Homeland Security also issued a statement to clarify that all individuals, regardless of immigration status, should receive the COVID-19 vaccines, and that it will not carry out enforcement operations at or near health care facilities, except in the most extraordinary circumstances.
The administration has launched several initiatives focused on addressing inequities in maternal health. In April 2021, President Biden issued a proclamation to recognize the importance of addressing the high rates of Black maternal mortality and morbidity. In addition, the Centers for Medicare and Medicaid Services (CMS) has approved several state waivers to extend the Medicaid postpartum coverage period, a policy which will become available as a state option beginning in 2022, under the American Rescue Plan Act. The Human Resources and Services Administration has also announced $12 million in awards for the Rural Maternal and Obstetrics Management Strategies Program, which is designed to develop models and implement strategies to improve maternal health in rural communities.
Looking Ahead
In sum, disparities in health and health care for people of color and underserved groups are longstanding challenges. The COVID-19 pandemic has exacerbated these disparities and heightened the importance of addressing them. Health disparities are driven by underlying social and economic inequities that are rooted in racism. Addressing disparities is important not only from a social justice standpoint but for improving our nation's overall health and economic prosperity. The federal government has identified equity as a priority and launched a range of initiatives to address disparities both in response to COVID-19 and more broadly. States, local communities, private organizations, and providers also are engaged in efforts to reduce health disparities. A broad range of efforts both within and beyond the health care system will be instrumental in advancing equity, including: prioritizing equity across sectors; providing resources to support efforts to advance equity; increasing availability of data; supporting and building on existing community strengths and resources; establishing incentives, accountability, and oversight for equity; and recognizing and addressing racism as a root cause of disparities.
Source: https://www.kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/
0 Response to "The Burden of Health Disparities Continues to Affect Disproportionately Which Population S"
Post a Comment